Lowering Hospital Readmissions through Remote Patient Monitoring of Post-Acute Patients
![]()
_____________________________________________________________________
By David Sheon

One of the less known policies of the Affordable Care Act, the Hospitals Readmission Reduction Program, requires that hospitals with higher than national average readmission rates for certain medical conditions and surgical procedures be penalized. For many hospitals, the readmission penalties result in millions of dollars in profit lost.
A recent Wall Street Journal article shines a light on remote patient monitoring and post-acute care coordination, a service that is experiencing rapid growth and focusing on readmission rate reduction. The service not only helps more people recover successfully from hospital stays, but it also keeps costs down for payers and helps hospitals avoid the risk of growing penalties.
According to an October 2014 article from Kaiser Health News, “Medicare is fining a record number of hospitals – 2,610 – for having too many patients return within a month for additional treatments, federal records released {recently} show. Even though the nation’s readmission rate is dropping, Medicare’s average fines will be higher, with 39 hospitals receiving the largest penalty allowed.”
********************************************************************************
A note from our sponsor: Are you, or is someone you love, an MS patient on Medicare in need of financial assistance? Click here to visit The HealthWell Foundation’s eligibility page.
********************************************************************************
Leading manufacturers of remote-monitoring equipment include Medtronic Inc., Philips NV and St. Jude Medical Inc., according to the Wall Street Journal article. Sales are expected to total about $32 billion this year, with a compound annual growth rate of 9.2% between 2014 and 2019.
In addition to addressing readmissions, effective remote monitoring represents an outstanding care redesign technique that can be implemented as part of a CMS bundled payment initiative, or as part of the quality program of an accountable care organization or clinically integrated network. The benefits accrue well beyond avoiding the penalties.
“The remote monitoring technology and implementation drives revenue issues beyond the CMS readmission penalties,” said John Kirsner, Partner, Jones Day, an expert on the implications of the ACA on hospitals. “In addition to the penalty avoidance component, this technology can assist in creating shared savings that result in additional topline revenue enhancement.”
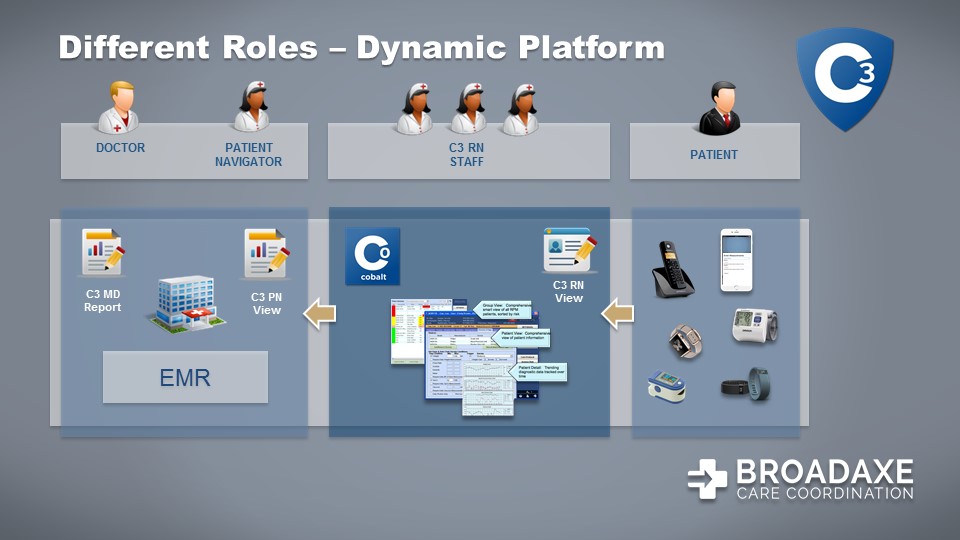
Some remote monitoring programs are further along than those mentioned in the Wall Street Journal article. For instance, over a year and half ago, Broad Axe Care Coordination and University of Virginia Health System (UVA) partnered to design and execute a comprehensive platform combining services and technology to reduce readmissions for key conditions where Medicare was imposing penalties, including heart attack, heart failure, pneumonia and COPD. Because of the success of the program and Medicare’s expansion of the penalty conditions, Broad Axe expanded its service at UVA to remotely monitor patients who had total joint replacements as well. The result for UVA has been a dramatic decrease in joint readmission rates, and a ready for prime time remote monitoring/care coordination program that can be put into place at hospitals across the country.
The system, called C3 at UVA, is a remote care management platform that combines telehealth services from experienced clinicians with robust analytics and an IT platform integrated with the health system’s EMR to provide UVA with a fully-outsourced care coordination solution.
“Broad Axe offered us something unique: a care coordination center that combines outstanding technology with dedicated clinicians — RNs, LPNs, and CNAs — to deliver ongoing care transition and care coordination services,” said Amy L. Tucker, MD, Associate Professor of Cardiovascular Medicine, University of Virginia Health System. “We’ve seen a great impact on the readmission rate.”
UVA and Broad Axe work together to look closely at those patients who are readmitted to see if the program can be further optimized.
For example, C3 can track not only readmission but when patients have follow-up visits. The system also can help to ascertain whether patients are following their medication instructions. This provides important feedback to see what areas of opportunity are most important for the health system to target to improve patient care.
Broad Axe executives are pleased with readmission rate performance between 25 and 45 percent below historical benchmarks, depending on the condition and payer population, and the associated penalty savings for the hospital.
“Historically, the adoption of remote monitoring technology has been stymied by the lack of financial incentives to use the technology,” said Scott Edelstein, also a Partner at Jones Day, specializing in regulated medical technologies. “Recent CMS initiatives such as the Hospital Readmissions Reduction Program and new reimbursement codes for remote chronic care management are fueling a renewed interest in this technology. This should create significant opportunities to increase access to, and quality of, care while lowering costs.”
Do you work in a hospital consider remote monitoring? What are your concerns? Or are you a recent patient who has participated in remote monitoring? www.RealWorldHealthCare.org welcomes your feedback.
To read this on the RWHC Blog, click here.

