




The Mechanics of Melanoma
May is Melanoma Awareness Month. This article originally appeared in the Biotech Primer WEEKLY. For more on the science behind the headlines, subscribe.
Melanoma 101

Emily Burke, BiotechPrimer.com
Melanoma accounts for less than one percent of skin cancer cases, yet accounts for the vast majority of skin cancer deaths (skincancer.org). If detected early enough, melanoma is almost always curable. If it is not detected early, it is likely to spread to other parts of the body, where it is more difficult to treat. It’s estimated that in 2017, there will be 87,110 new cases of melanoma in the U.S., and 9,730 melanoma-related deaths (Aim at Melanoma Foundation). Melanoma is one of the types of cancers most common in young adults, with 25 percent of new cases occurring in people under age 45. Its prevalence is growing – the number of new cases/year relative to the total population has doubled since 1973.
In this column, we’ll review the basics of melanoma, and discuss the latest new therapies recently approved and in development.
Melanoma’s Method
Melanoma is the uncontrolled growth of the pigment-producing cells known as melanocytes, which are located in the bottom layer of the skin’s top layer (the epidermis). Like other types of cancers, melanoma arises from gene mutations in these cells that impact cell growth and division. In the case of melanoma and other skin cancers, the DNA damage is usually caused by ultraviolet (UV) radiation, resulting in a tumor that initially grows in the skin, spreading along the epidermis. If the melanoma is detected at this stage, it can often be surgically removed. If the out of control cell growth is not caught in these early stages, it penetrates deeper layers of the skin, eventually coming into contact with lymph and blood vessels which enable it to spread to other parts of the body. When the melanoma reaches this stage, it is called metastatic melanoma.
Although anyone can get melanoma, fair-skinned people are at higher risk for all types of skin cancer, since increased skin pigmentation helps to block the damaging UV rays from penetrating and damaging skin cell DNA. However, darker-skinned people can and do get skin cancer, and thus should also be vigilant about sun protection.
Atypical moles have also been linked to an increased risk of melanoma. Moles are clusters of melanocytes, and there is a slightly increased risk of melanoma arising within these clusters. Of course, most moles are harmless and do not lead to melanoma. However, any sudden changes in the color, shape, or size of a mole should be evaluated by a doctor.
Genetic Factors: p53 & BRAF
Although most cases of all types of skin cancer are traceable to excessive sun exposure, about 10% are likely due to genetic factors. The gene most commonly mutated in familial melanoma is p53. p53 is a “tumor suppressor,” which means that it detects DNA damage in cells, and triggers either DNA repair pathways or activates cell death if the DNA damage cannot be repaired. Another gene, known as the BRAF gene, regulates cell growth and is mutated in inherited forms of melanoma. About half of all genetically-based melanomas have the BRAF mutation.
Let’s take a closer look at BRAF. BRAF codes for a protein required for the transmission of a growth signal from a cell surface receptor to the cell nucleus (growth signal transduction). Growth signaling is initiated by a growth factor binding to its receptor. This binding transmits a signal through the membrane, causing the internal portion of the receptor to interact with and activate a protein inside of the cell. This activation is then transferred to the next protein in the pathway, and so on until the signal reaches the last protein in the pathway. When this protein is activated, it enters the nucleus, where it turns on specific genes that make proteins which initiate cell division. BRAF is one of the proteins in this pathway. In BRAF-associated melanoma, the mutated BRAF is always turned on even when no growth factor is present.
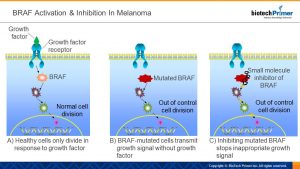
Small molecule drugs that inhibit overactive BRAF have been developed and approved for the treatment of late-stage melanoma.
Immunotherapies in the Fight
A few different checkpoint inhibitor therapies have been approved to treat metastatic melanoma. These are drugs that enable killer T-cells – immune system cells that recognize and kill threats such as cancer cells – to become fully active against a tumor cell target. These drugs target inhibitory proteins on the surface of T-cells such us CTLA-4 and PD-1. These proteins act as “off switches” for killer T-cells. By inhibiting these off switches, the killer T-cells become fully activated, and able to target and kill melanoma cells.
A second type of immunotherapy that has been approved for melanoma is an oncolytic virus therapy. An oncolytic virus is a virus that infects and kills cancer cells. The cancer cells are killed through cell lysis – as the virus multiplies inside of the cells, it causes them to burst open. This in turn releases new infectious particles that can target remaining tumor cells. In addition to direct killing of cancer cells via lysis, the presence of an actively replicating virus helps to activate the patient’s immune response to target the area.
In the Pipeline
A new type of immunotherapy drug is in Phase 3 clinical development. The drug is a small molecule inhibitor of the enzyme IDO1. IDO1 helps regulatory T-cells to develop and become activated. Regulatory T-cells suppress the immune response, and therefore help cancer cells to escape immune surveillance. Inhibiting IDO1 should suppress the development of regulatory T-cells, bolstering the immune response against melanoma.
Implications of microRNA
Last year, researchers at Tel Aviv University published a report describing how melanoma metastasizes. Their work suggests that melanoma cells release tiny vesicles that contain microRNA, a type of regulatory RNA produced by all cells. These micro-RNA filled vesicles induce changes in the dermis – the layer of skin just below the epidermis where the melanoma begins. The dermis contains blood vessels, and thus a pathway for metastasis. The changes in the dermis induced by the small vesicles released from the melanoma cells makes the cancer cells able to access those blood vessels. The Tel Aviv team is identifying drug candidates that may interfere with this process, preventing the metastasis that makes melanoma so deadly.
The best strategy for melanoma remains prevention and proactive monitoring – limiting sun exposure and monitoring the skin for any unusual growths or changes in moles. Increased understanding of the molecular pathways that contribute to melanoma’s development and spread will provide physicians with additional tools to fight those cases of metastatic melanoma that inevitably will continue to arise.

