




Spotlight on Macular Degeneration
Editor’s Note: The following article is reprinted with permission from the Biotech Primer WEEKLY newsletter.
Spotlight on Macular Degeneration

Emily Burke, BiotechPrimer.com
Getting old is for the birds. Time has its way with nearly every part of us: skin, hair, muscles. Few changes are more alarming, however, than those to our eyes. There’s more to old eyes than bifocals and cataracts though. One of the most common eye diseases is age-related macular degeneration (AMD). It affects more than 13 million people over age 50 in the United States. It’s the leading cause of vision loss in this age group.
Eyes are spectacularly complicated organs: they contain over two million moving parts. You know some of the basics: iris, pupil, lens, retina. In some ways, this last, the retina, is more accurately considered part of the brain.
Term of the Week: Retina
The retina is composed of light-sensitive nervous tissue which forms a thin membrane that lines the rear two-thirds of the eyeball. It takes in light from the world around and converts into neural signals that travel along the optic nerve to the brain, telling us — “Hey, there’s an apple, or a laptop, or whatever.”
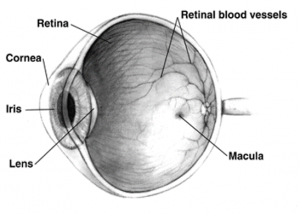
The anatomy of the eye (The National Eye Institute)
The macula is the small central area of the retina that enables central, high-resolution, color vision.
Macular Degeneration: A Gradual Loss of Vision
Macular degeneration progressively devastates eyesight, causing blurred vision and blocking the center of a person’s visual field. What begins as a minor annoyance ends up making everyday tasks such as reading and driving impossible.
Ophthalmologists and other scientists don’t know exactly what causes AMD. It is however, associated with a buildup of proteins and lipids just beneath the retina. These deposits, drusen, are a normal part of aging. However, the presence of larger or more drusen raises the risk of AMD. As the disease progresses, vision decreases. There are two types of AMD: neovascular (wet) or atrophic (dry).
Wet Age-Related Macular Degeneration (AMD)
In wet AMD, the infiltration of excess blood vessels is the main culprit. These abnormal vessels often leak fluid and blood, injuring the retina. Wet AMD progresses quickly, leading to loss of central vision without treatment. This form of the disease accounts for about 10 percent of cases.
FDA-approved treatments for wet AMD include Ranibizumab, Brolucizumab, and Aflibercept. These work by mopping up excess vascular endothelial growth factor (VEGF), which is what causes the excess blood vessel growth. Ranibizumab and Brolucizumab are monoclonal antibodies specific for VEGF. Aflibercept consists of the VEGF-receptor fused to the constant region of an antibody for stability. Similar to a mAb, this combination is called a fusion protein. It’s highly specific for VEGF, binding it before it reaches its intended receptor on the surface of blood vessels. These VEGF-blocking treatments effectively stop the progression of AMD, but don’t cure it.
KS-301 is an antibody-biopolymer conjugate (ABC), which also targets VEGF. An ABC is an antibody with a biopolymer—a chain of repeating subunits produced by a living organism—attached. In KS-301, the repeating subunits are lipids. They make the antibody more stable. That means patients can go up to five months between injections, compared to one month (Ranibizumab), two months (Aflibercept), or two to three months (Brolucizumab). The treatment is now in Phase II/III development.
These therapies are injected in the patient’s eye, which makes them understandably unappealing. As an alternative, PAN-90806 is a small molecule inhibitor of VEGF that patients can administer at home by eyedrop. The drug has completed Phase I clinical studies.
It may be possible to do away with repeated treatments altogether with gene therapy. RGX-314 delivers a gene encoding an anti-VEGF antibody. In Phase I/II studies, participants produced the therapeutic protein, which controlled VEGF levels.
Dry Age-Related Macular Degeneration (AMD)
Dry AMD involves a gradual breakdown in the macula’s light-sensitive cells. The dry variety progresses much more slowly than wet and accounts for about 90 percent of AMD cases. Advanced dry AMD occurs when cells in regions of the retina have wasted away and died. Sometimes these regions of atrophy (death) look like a map to the physician who is examining the retina, giving rise to the term “geographic atrophy” for late-stage dry AMD.
Currently, no treatments exist for dry AMD. However, some studies suggest that high doses of antioxidants including C and E vitamins, copper, zinc, and beta-carotene may slow its progression.
Inflammation, specifically the activation of complement proteins, is associated with drusen buildup and dry AMD progression. When they’re activated, these immune system proteins interact, destroying targeted cells. Inappropriate activation of complement proteins can result in the destruction of healthy cells and tissue. A number of drugs in clinical development work by inactivating complement proteins:
- APL-2 is a peptide drug in Phase III development. APL2 binds to complement protein C3 and prevents its interaction with other complement proteins. Preventing this interaction prevents activating their destructive power.
- Avacincaptad pegol is a DNA aptamer in Phase II development. DNA aptamers are short strands of DNA that bind to a specific protein. Avacincaptad pegol binds to and inhibits complement protein C5.
- IONIS-FB-LRx is an antisense drug that blocks the production of complement factor B, currently in Phase II clinical testing.
Last month, the National Eye Institute announced preparations to begin clinical testing of stem cells for dry AMD. In the lab, researchers have coaxed stem cells to grow into retinal cells. In rodent and pig models, these cells restored vision, setting the stage for test human testing.
About Biotech Primer Inc.
Biotech Primer Inc. delivers current, relevant training to help professionals understand the science, business and regulatory processes essential to the biotechnology, pharmaceutical, molecular diagnostics and medical device industries. For more information, visit www.biotechprimer.com.

